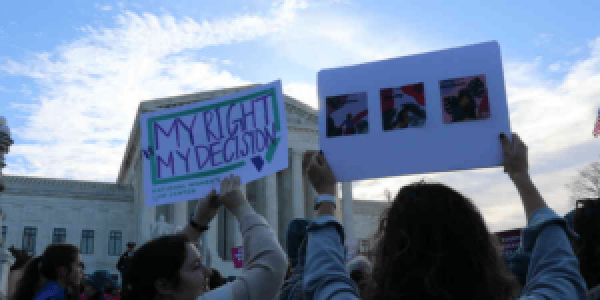
Abortion rights, women of color, and LGBTQI+ people are under attack. Pledge to join us in fighting for gender justice.
 Women of color confront systemic discrimination–on the basis of race, gender, and other characteristics like sexual orientation, gender identity, immigration or disability status–throughout their lives. It is important to understand that multiple and compounding forms of discrimination experienced over a lifetime can have a devastating impact on the economic security and health of older women of color. Without policies that specifically address the needs and well-being of older women of color, they will bear the burden of a lifetime of disparities.
Women of color confront systemic discrimination–on the basis of race, gender, and other characteristics like sexual orientation, gender identity, immigration or disability status–throughout their lives. It is important to understand that multiple and compounding forms of discrimination experienced over a lifetime can have a devastating impact on the economic security and health of older women of color. Without policies that specifically address the needs and well-being of older women of color, they will bear the burden of a lifetime of disparities.
Methodology: The data cited throughout this report comes from multiple sources, including the U.S. Census Bureau, the Social Security Administration and other federal agencies, numerous surveys, as well as analyses of these and other data conducted by other individuals and organizations.
In this issue brief, we use the general term “older,” rather than a specific age range. Different age ranges are used in different data sets utilized in this issue brief, and for the purposes of different federal programs and laws. For example, the Age Discrimination in Employment Act protects individuals ages 40 and older against age discrimination.1 Please refer to individual source notes for information about the relevant age categories or ranges.
Within these multiple data sources, moreover, there are a wide range of terms used to refer to people of different racial or ethnic groups. In this brief, we use the following terms to refer to women and households: Asian, Black, Latina/x, Native American, and white, non-Hispanic because these terms most closely align with the categories found in the Census and SCF surveys. The “Asian” race category includes those who identified themselves as Asian in the U.S. Census Bureau. While we use “Asian” rather than “Asian American and Pacific Islander” (AAPI) throughout because it best reflects the data, we want to acknowledge that the failure to disaggregate AAPI people by more specific ethnicity obfuscates the diversity of this community.2 The “Black” race category includes those who identified themselves as Black or African American. The “Latina” category includes women of any race who identified themselves to be of Hispanic, Latino, or Spanish origin. We use the term “Latinx” to discuss households of any race who are of Hispanic, Latino, or Spanish origin because this term allows for more gender inclusivity. The “Native American” race category includes those who identified themselves as American Indian or Alaskan Native. The “white, non-Hispanic” race category includes those who identified themselves as white, but not of Hispanic, Latino, or Spanish origin. Please refer to each individual source note for more information on racial and ethnic categories.
The Economic Security of Older Women of Color
Older women face a significant challenge as they attempt to maintain their economic security as they age. Their economic security hinges on what they have available in both income and savings, yet women, and women of color in particular, face deep inequities in the workforce, economy, housing and health care systems that constrain both. The cumulative impact of a lifetime of disparities means that, even before the additional burdens brought on by COVID-19, the risk of economic insecurity only increases for older women of color.
In every age group, including among older adults, women typically make less than men, which generates less available income and savings in retirement as compared to men.3 The gender wage gap alone can cause women to lose $400,000 over a 40-year career, with the lifetime loss of earnings for Black women totaling nearly $1 million, and the lifetime earnings loss for Latinas exceeding $1.1 million.4 Lower earnings result in lower Social Security benefits, which for workers’ benefits is currently based on their lifetime earnings over a 35-year period. When combined with disparities in retirement savings, older women have less available income overall to live on during retirement and are significantly more likely than men to end up living in poverty. And poverty rates for older Black, Native American, and Latina women are more than twice that of older white women.5 Women who are divorced, widowed, or never married are particularly at risk of falling into poverty.6
Women are also more likely to provide caregiving that takes them away from wage-earning work for significant portions of their lives, which also negatively impacts their ability to increase their earnings or build up their savings. A 2013 AARP report found that, among people aged 45-74, women were three times more likely than men to quit their jobs due to caregiving.7 Fewer years in the workforce, combined with lower pay as discussed above, ultimately impacts the amount women receive from Social Security. While the average Social Security retirement and survivor benefit for men in 2019 (excluding disability benefits) was $1,612, it was only $1,283 for women.8 For some women, no real “retirement” is feasible because they need to keep working into old age to pay for basics like food and housing.
In fact, older women can still struggle with housing instability and are at greater risk of food insecurity.9 A lack of affordable housing, for example, has led to older adults experiencing greater rental cost burdens, increasing their risk of eviction and homelessness, and forcing them to use more of their income on housing at the expense of other necessities such as food and medicine.10 While housing programs run through the Department of Housing and Urban Development (HUD), such as Section 202 supportive housing for the elderly, provide affordable housing to low-income households, these programs do not provide assistance for all people who are eligible. Less than a quarter of all eligible households receive rental assistance. Yet older women constitute almost three-quarters of those who receive Section 202 housing, highlighting the need for housing support among low-income older women in particular. Older women also struggle disproportionately with food insecurity, making up 62% of all adult SNAP participants ages 60 and older.11
In addition to these factors and the effects of systemic discrimination, economic downturns such as the Great Recession and the COVID-19 recession can devastate the income and savings of many older women even further. Women of color are overrepresented in the front-line workforce,12 and sectors in which women workers predominate suffered heavy job losses during the COVID-19 recession.13 While women’s overall unemployment rate dropped to 4.8% in August, nearly 1 in 13 Black women (7.9%) and nearly 1 in 17 Latinas (6.0%) remained unemployed.14 Nearly 1.6 million women have left the workforce since February 2020,15 many because they cannot simultaneously work and meet caregiving responsibilities.16 In May 2021, 124,000 fewer Black women17 and 64,000 fewer Latinas18 ages 55 and older were in the labor force compared to February 2020. According to a recent NWLC analysis of the U.S. Census Bureau’s Household Pulse Survey, nearly one in four Latinas and Black, non-Hispanic women were in a household that has lost employment income in the last month.19
Job losses not only result in loss of income in the short term, but reduce lifetime earnings, cause people to deplete existing savings and forestall retirement savings, and delay the accrual of credits for future Social Security retirement benefits. Research showed that older adults who lost their jobs during the Great Recession also had to deal with the challenge of finding new employment in the face of age discrimination, which can make it more difficult for older workers, especially women and people of color, to get hired into new jobs that are comparable to their previous positions.20 Instead, older workers may either face extended periods of unemployment during their prime earning years or be forced to retire earlier than anticipated.21 Those who decide to claim Social Security early retirement because of the difficulty of finding new work are forced to accept a permanently lower retirement benefit, further reducing the retirement income available to them as they age.
Time will tell what additional negative long-term effects the COVID-19 pandemic will have on the lifetime incomes, wealth, and overall economic security of women of color – who experience more detrimental impacts and recover more slowly from recessions.22 For example, during the Great Recession, the loss of home equity was a particularly heavy blow for older women, and single Black and Latina women especially. Research found that older adult single women who could not keep their homes during the Great Recession lost 100% or more of their total wealth.23
Ways to support older women of color and improve their economic security
The story does not end with older women falling into poverty in the face of numerous challenges to their economic security over time. Instead, we can implement policies that recognize both the contributions that women have provided to society throughout their lives, and the various types of discrimination, including racial, ethnic, and gender-based inequities that have negatively impacted their overall income and savings. The short-term relief in the American Rescue Plan Act and other COVID relief legislation is not enough to ameliorate the immediate and longer-term impacts of the pandemic and the longstanding inequities impacting the economic security of older women.
Improving Data Collection
One critical first step is improving our collection of data on the well-being of older women, and in particular older women of color. Data that combines information about all older adults as a monolith and fails to disaggregate information for older adults by race and sex, can paint an unrealistic picture of the status of older women and masks the harmful impacts of discrimination at the intersection of race and gender. This makes it difficult to identify the problems most pressing for older women and to create and implement relevant policies that effectively address them.
Redefining Economic Security
We should also redefine what it means to be economically secure in our society. Simply having income above the poverty level is insufficient. The federal poverty level for a household of one, at just $12,880 per year, or $1,073 per month, is so low that almost no one could actually afford to live in dignity on this minimal amount of income. The Elder Index is a tool that calculates the amount of income an older adult would actually need, taking into account geographic location, to meet their basic needs for housing, health care, food, and other essentials. The national average is more than twice the federal poverty rate, indicating that current programs must do more to actually help older adults, and older women, truly achieve economic security.
Expanding Key Income Supports
We must also expand federal and state benefits, including Social Security, SSI, SNAP, refundable tax credits like the Earned Income Tax Credit, and housing assistance programs for low-income older adults so that they have the income and resources to actually meet their needs. The Social Security program, which looks only at wage-earning work, should be expanded to include the work of caregivers in its calculation of benefits so that older women who have taken time away from the official workforce are still compensated in retirement for the value of the unpaid caregiving they provided. We should also increase Social Security and Supplemental Security Income (SSI) benefits so that the minimum benefit level is above the (already too low) federal poverty level. SSI is an important federal companion to Social Security, and also administered by the Social Security Administration, that provides cash assistance to very low-income older adults and people with disabilities who do not receive significant income through Social Security Retirement, Survivors, or Disability Insurance. At only $794 per month in 2021, the maximum SSI benefit is less than 75% of the federal poverty level, leaving older adults to struggle to meet their basic needs despite qualifying for the program. Amendments to the program proposed in legislation such as the Social Security Restoration Act of 2021 would not only increase SSI benefits, but would also modernize the SSI program to update rules that haven’t been changed in over 40 years, and ensure that eligible low-income older adults and people with disabilities were better able to access the program.
SNAP improvements can also help reduce food insecurity among older women of color. For example, shifting from the Thrifty Food Plan to the Low-Cost Food Plan will boost the value of benefits and help them last through more of the month. USDA can also establish standardized excess medical deductions for older adults and people with disabilities to overcome burdensome verification requirements. Additional funding for outreach and streamlining SNAP application processes would also help more older women of color access SNAP.
Our housing policies must include a plan to provide affordable housing to all those who need it. The Housing is Infrastructure Act of 2021 (H.R.2421),24 would provide significant federal investments to preserve and create more deeply affordable and accessible housing. We must increase the stock of affordable housing so that there are enough rental units available to meet the needs of low-income renters, including seniors. We should also increase funding for housing assistance programs. Legislation such as the Ending Homelessness Act of 2021 (H.R.4496),25 for example, would create a universal housing voucher program available to every eligible renter. We should consider the particular needs of older renters, providing the accessible housing and linked services that allow low-income older adults to age in place, remaining close to their friends, families and communities.
Health Care of Older Women of Color
Older women face significant challenges to their health and wellbeing. Deep inequities in our workforce, housing, and economy, as discussed above, result in increased economic insecurity, chronic stress and access to fewer resources over a woman’s lifespan. These inequities compound and compromise the health of women of color, and women broadly, as they age. Higher health needs and lower financial resources also cause women, particularly women of color, to forgo and deny themselves care at higher rates than men. These inequities can have devastating consequences for women’s health.
Older women bear the burden of higher health care costs. A significant portion of out-of-pocket spending for older women is for services not covered by Medicare. A woman who is 65 years of age will spend approximately $47,000 more in retirement for health care expenses than her male counterpart.26 Women 85 and over spend an average of $8,574 on services and premiums while men spend on average $7,399.27 Disparities in costs are likely to continue to widen in future years due to rising health care inflation and differences in life expectancies so that a 45-year-old woman today will pay 27.5% more for health care through premiums alone compared to her male counterpart during retirement.28
Higher costs can be attributed to a variety of factors including longer life expectancy and increased expenditures related to chronic condition management. Women are more likely than men to have a chronic condition and more likely to have more than one chronic condition.29 The prevalence of chronic conditions only increases with age30 and medication is often a vital part of chronic condition management. As a result, medication usage among women also increases with age. Seventy-two percent of women ages 50-64 take at least one medication on a regular basis compared to only 42% of women ages 18-49.31
These costs are particularly burdensome to Black, Native American, and Latina women, as they are more than twice as likely as older white women to live in poverty.32 Black women, in particular, are harmed by the costs of chronic condition management. Black women are more likely than other racial and gender groups to experience chronic diseases, including heart disease, stroke, diabetes and cancer33 yet have fewer financial resources to treat these conditions as they age.
The COVID-19 pandemic makes the need for equitable resources and support all the more urgent. Older women not only faced elevated risk for severe illness and fatality from COVID-19,34 they also faced the greatest risk of developing long-term, and potentially debilitating, after-effects from the virus.35 Yet, older women were less likely to get COVID-19 vaccines than older men36 and more likely to have gone without needed health care during the pandemic as compared to men.37 This forgoing of care led to reduced screenings, reduced compliance with care plans and reduced overall health.38 Finally, older women living alone, especially older women with mobility problems, experienced decreased access to food, medicine, and other supports from loved ones. We do not know the full extent of the health consequences to older women, but what is known, is that immediate and decisive action is required.
Ways to support older women of color and improve their health and wellbeing
Expanding Eligibility for Medicaid and Medicare Savings Programs
Medicaid plays a critical role for older women by providing access to vital services that Medicare does not pay for, including long-term services and supports and transportation. Medicaid is also crucial in making Medicare more affordable for low-income recipients. Through Medicare Savings Programs (MSPs), Medicaid pays for the costs associated with Medicare, including premiums and cost sharing. Unfortunately, current MSP income eligibility and resource limits in most states force aging adults and people with disabilities to live in poverty to access care.39
Although low-income women may be dually covered by Medicare and Medicaid, states’ variation in Medicaid benefit packages and Medicare’s lack of coverage for basic services like dental, vision, and hearing leaves many dual beneficiaries with burdensome out-of-pocket costs, which can greatly press budgets of older women with fixed incomes, few financial resources, and other financial obligations. States have the option to set their Medicaid eligibility income and resource limits to allow older women to access critical health care benefits while also maintaining enough income to cover basic needs and save for an emergency.
California, for example, has raised its income limit for its aged and disabled program to 138% of the federal poverty limit and just approved a policy to eliminate its resource limit, and Arizona has eliminated its resource limit entirely for older adults and people with disabilities.40 Similarly, states can expand access to MSPs so that more older women could reduce their out-of-pocket spending on health care. For example, Alaska, Connecticut, the District of Columbia, Hawaii, and Maine have higher income limits. Alabama, Arizona, Connecticut, Delaware, DC, Mississippi, New York, and Vermont have eliminated using resources beyond their earnings and other income to determine eligibility.41
Investing in the Paid Care and Home and Community-Based Services Infrastructure
The COVID-19 pandemic made clear how critical it is that we invest in our home and community-based care infrastructure. More than 184,000 residents in shared living communities died from COVID-19, with disproportionately higher rates of deaths occurring in nursing homes with more residents of color.42,43 Most older women do not want to reside in a facility to receive their care. Instead, most want to age in their homes and communities and remain as independent as possible. Paid caregiving and home and community-based services (HCBS) allow older women to do just that.
Medicaid is the primary payer for HCBS. Unfortunately, however, while Medicaid coverage for care in a nursing home is guaranteed if you are otherwise eligible, care or services provided at home or in the community are not. Making HCBS an entitlement equal to nursing facility coverage is essential for older women of color to stay in their homes and maintain ties to their communities. The optional structure of HCBS leads to significant disparities in access to services depending on what state you live in, your, age, your disability, and your race.44 As a result, women of color are harmed across generations. Without access to HCBS, older women of color are forced to receive the care they need in a nursing facility. Alternatively, they rely on their family to fill in the gaps–most often their daughters, who risk falling into poverty themselves when they either cease or reduce their paid work to act as a caregiver.
Even when HCBS is available, research has found that there are disparities in the number of services rendered. Though women are more likely to access HCBS services and to have worse health indicators than men,45 more money is spent on services for men.46 For women of color, race compounds this disparity. One study found that HCBS expenditures were disproportionately higher for white women than Black women.47 Another study found that Black HCBS users received less case management, equipment, technology and modification services, and nursing services compared to whites.48
To address these inequities, HCBS enrollment and expenditures data must be collected by race, gender and disability, cross-tabulated and released consistently. Further, once specific inequities are identified, policies must be crafted to address barriers and bias and achieve equitable enrollment and expenditures.
Expanding Medicare Benefits
In addition to expanding access to Medicaid HCBS and MSPs, expanding the benefits Medicare covers is necessary to ensure lower-income women who are not eligible for Medicaid can afford care. By including coverage for oral health, vision and hearing, older women will have these unmet basic medical needs covered by Medicare, eliminating high out-of-pocket medical expenses that contribute to their economic insecurity. Adding these benefits to Medicare would also act to reduce health disparities since women—and particularly women of color—are more likely to be low-income and unable to access these services.49
Conclusion
Now more than ever, it is critically important to invest in the economic security and health of women of color.
1 29 U.S.C.A. § 621 (2021).
2 See Nat’l Asian Pacific Am. Women’s Forum, Still Fierce, Still Fighting: A Reproductive Justice Agenda for Asian Americans and Pacific Islanders 3 (2017), https://www.napawf.org/uploads/1/1/4/9/114909119/stillfiercestillfighting.pdf.
3 Heidi Hartmann, What It’s Worth 285-299 (Laura Choi et al. eds., 2015).
4 See, e.g., Jasmine Tucker, Nat’l Women’s Law Ctr., The Wage Gap Has Robbed Women of Their Ability to Weather COVID-19 (March 2021), https://nwlc.org/wp-content/uploads/2021/03/EPD-2021-v1.pdf.
5 Amanda Fins, Nat’l Women’s Law Ctr., National Snapshot: Poverty among Women and Families, 2020 (December 2020), https://nwlc.org/wp-content/uploads/2020/12/PovertySnapshot2020.pdf; Juliette Cubanski, Wyatt Koma, Anthony Damico, & Tricia Neuman, Kaiser Family Found., How Many Seniors Live in Poverty? (Nov. 2018), https://files.kff.org/attachment/Issue-Brief-How-Many-Seniors-Live-in-Poverty.
6 Social Security Admin., Marital Status & Poverty (May 2016), https://www.ssa.gov/policy/docs/population-profiles/marital-status-poverty.html.
7 Rebecca Perron, AARP, Staying Ahead of the Curve 2013: The AARP Work and Career Study (Jan. 2014), https://www.aarp.org/content/dam/aarp/research/surveys_statistics/general/2014/Staying-Ahead-of-the-Curve-2013-The-Work-and-Career-Study-AARP-res-gen.pdf.
8 Social Security Admin. Annual Statistical Supplement, 2020 (last visited Sep. 23, 2021), https://www.ssa.gov/policy/docs/statcomps/supplement/2020/5a.html.
9 Simone G Fernandes et al., Food Insecurity in Older Adults: Results from the Epidemiology of Chronic Diseases Cohort Study 3, 5 Frontiers Med. 203 (2018), doi:10.3389/fmed.2018.00203.
10 Patti Prunhuber & Vivian Kwok, Low-Income Older Adults Face Unaffordable Rents, Driving Housing Instability and Homelessness (Feb. 2021), https://justiceinaging.org/wp-content/uploads/2021/02/Older-Adults-Rental-Housing-Burdens.pdf.
11 U.S. Dep’t of Agriculture, Food, & Nutrition Serv., Off. of Pol’y Support, Characteristics of Supplemental Nutrition Assistance Program Households: Fiscal Year 2019 (2021), https://fns-prod.azureedge.net/sites/default/files/resource-files/Characteristics2019.pdf.
12 Nat’l Women’s Law Ctr., Women Make Up the Majority of Front Line Workers of the COVID-19 Crisis (March 2020), https://nwlc.org/wp-content/uploads/2020/05/final_NWLC_Frontlines_FactSheet-002.pdf.
13 See, e.g., Amanda Fins, Nat’l Women’s Law Ctr., COVID-19 and the Ensuing Recession Puts Women in Retail at Risk (July 2020), https://nwlc.org/resources/covid-19-and-the-ensuing-recession-puts-women-in-retail-at-risk/; Claire Ewing-Nelson, Nat’l Women’s Law Ctr., One in Five Child Care Jobs Have Been Lost Since February, and Women Are Paying the Price (August 2020), https://nwlc.org/resources/one-in-five-child-care-jobs-have-been-lost-since-february-and-women-are-paying-the-price/; Claire Ewing-Nelson, Nat’l Women’s Law Ctr., More Than Three in Four of the Health Care Workers Fighting COVID-19 Are Women (August 2020), https://nwlc.org/resources/more-than-three-in-four-of-the-health-care-workers-fighting-covid-19-are-women/.
14 Jasmine Tucker, Nat’l Women’s Law Ctr., At August’s Rate, It Will Take Women 9 Years to Regain the Jobs They Lost in the Pandemic (September 2021), https://nwlc.org/resources/at-augusts-rate-it-will-take-women-9-years-to-regain-the-jobs-they-lost-in-the-pandemic/.
15 Id.
16 See, e.g., Paula Span, Family Caregivers Feel the Pandemic’s Weight, N.Y. Times (May 21, 2021), https://www.nytimes.com/2021/05/21/health/coronavirus-home-caregivers-elderly.html; Sarita Gupta, The Price We Pay: Why We Need To Redefine Care in America, Ford Found. (May 11, 2021), https://www.fordfoundation.org/just-matters/just-matters/posts/the-price-we-pay-why-we-need-to-redefine-care-in-america/?utm_source=grantees&utm_medium=social&utm_campaign=Care_Fund&s=03; Usha Ranji , Brittni Frederiksen, Alina Salganicoff, & Michelle Long, Kaiser Family Found., Women, Work, and Family During COVID-19: Findings from the KFF Women’s Health Survey (Mar. 21, 2021), https://www.kff.org/womens-health-policy/issue-brief/women-work-and-family-during-covid-19-findings-from-the-kff-womens-health-survey/; Katherine Ellison, Caregivers of Elderly Loved Ones Face Heavy Emotional, Physical, Financial Toll, Wash. Post (Sept. 27, 2020), https://www.washingtonpost.com/health/caretaker-stress-depression-anxiety-increases/2020/09/25/abd281f6-e933-11ea-97e0-94d2e46e759b_story.html.
17 NWLC calculation using Bureau of Labor Statistics (BLS), “(Unadj) Civilian Labor Force Level – 55-64 yrs., Black or African American Women” Labor Force Statistics from the Current Population Survey (Washington, DC: June 8, 2021), https://beta.bls.gov/dataViewer/view/timeseries/LNU01000463 and “(Unadj) Civilian Labor Force Level – 65 yrs. & over, Black or African American Women,” Labor Force Statistics from the Current Population Survey (Washington, DC: June 8, 2021), https://beta.bls.gov/dataViewer/view/timeseries/LNU01000465; see also Joint Econ. Comm., The Impact of the Coronavirus Recession on Older Workers (August 2020), https://www.jec.senate.gov/public/_cache/files/25a2a42f-6458-4d59-8c02-b19e6e0146f9/impact-of-the-coronavirus-recession-on-older-workers-final.pdf (noting that unemployment rates for older workers exceeded those for prime-age workers from March to July 2020).
18 NWLC calculation using Bureau of Labor Statistics (BLS), “(Unadj) Civilian Labor Force Level – 55-59 yrs., Hispanic or Latino Women,” Labor Force Statistics from the Current Population Survey (Washington, DC: June 8, 2021), https://beta.bls.gov/dataViewer/view/timeseries/LNU01000368 and “(Unadj) Civilian Labor Force Level – 65 yrs. & over, Hispanic or Latino Women” Labor Force Statistics from the Current Population Survey (Washington, DC: June 8, 2021), https://beta.bls.gov/dataViewer/view/timeseries/LNU01000371; see also Joint Econ. Comm., supra note 17.
19 Sarah Javaid & Jasmine Tucker, Nat’l Women’s Law Ctr., Women of Color Use Their Advance Child Tax Credit to Cover Food Costs (September 2021), https://nwlc.org/resources/women-of-color-use-their-advance-child-tax-credit-to-cover-food-costs/.
20 David Neumark, Ian Burn, & Patrick Button, Age Discrimination and Hiring of Older Workers, Fed. Reserve Bank of San Francisco (February 27, 2017), https://www.frbsf.org/economicresearch/publications/economic-letter/2017/february/age-discriminationand-hiring-older-workers/.
21 See, e.g., Joint Econ. Comm., supra note 17.
22 See, e.g., Jared Bernstein, Janelle Jones, Ctr. on Budget & Pol’y Priorities, Groundwork Collab., The Impact of the COVID-19 Recession on the Jobs and Incomes of Persons of Color (May 13, 2020), https://groundworkcollaborative.org/wp-content/uploads/2020/05/Groundwork-Bernstein-Jones-paper_5.13.pdf (stating that the incomes of low-paid workers are expected to decline precipitously, with the incomes of Black workers falling more, and even faster); Chandra Childers & Gladys McLean, Inst. for Women’s Pol’y Rsch., Black and Hispanic Women Lag in Recovering from the Recession (August 2017), https://iwpr.org/publications/black-hispanic-women-lag-recovering-recession/.
23 Amy Baker, Stacia West, & Anna Wood, Asset Depletion, Chronic Financial Stress, and Mortgage Trouble Among Older Female Homeowners, 59 Gerontologist 230 (2017).
24 The Housing is Infrastructure Act of 2021, H.R.2421, 117th Cong. (2021).
25 Ending Homelessness Act of 2021, H.R.4496, 117th Cong. (2021).
26 Bradley Sawyer & Gary Claxton, Kaiser Family Found. Analysis of Medical Expenditure Panel Survey, Agency for Healthcare Rsch. and Quality, U.S. Dep’t of Health and Human Serv’s, How Do Health Expenditures Vary Across the Population? (Dec. 2017), healthsystemtracker.org/chart-collection/health-expenditures-vary-across-population/#item-population-reports-good-better-health_2015.
27 Juliette Cubanski, Christina Swoope, Anthony Damico, & Tricia Neuman, Kaiser Family Found., How Much Is Enough? Out-of-Pocket Spending Among Medicare Beneficiaries: A Chartbook (Jul. 2014), kff.org/medicare/report/how-much-is-enough-out-of-pocket-spending-among-medicare-beneficiaries-a-chartbook/.
28 HealthView Services, The High Cost of Living Longer: Women and Retirement Income (Aug. 2017), https://hvsfinancial.com/download-the-high-cost-of-living-longer/.
29 Peter Boersma, Lindsey I. Black, & Brian W. Ward, Prevalence of Multiple Chronic Conditions Among U.S. Adults, 17 Preventing Chronic Disease 1 (2018), https://www.cdc.gov/pcd/issues/2020/20_0130.htm.
30 Id.
31 Michelle Long, Brittni Frederiksen, Usha Ranji, & Alina Salganicoff, Kaiser Family Found., Women’s Health Care Utilization and Costs: Findings from the 2020 KFF Women’s Health Survey (Apr. 2021), https://www.kff.org/womens-health-policy/issue-brief/womens-health-care-utilization-and-costs-findings-from-the-2020-kff-womens-health-survey/.
32 Amanda Fins, Nat’l Women’s Law Ctr., National Snapshot: Poverty among Women and Families, 2020 (Dec. 2020), https://nwlc.org/wp-content/uploads/2020/12/PovertySnapshot2020.pdf; Juliette Cubanski, Wyatt Koma, Anthony Damico, & Tricia Neuman, Kaiser Family Found., How Many Seniors Live in Poverty (Nov. 2018), https://files.kff.org/attachment/Issue-Brief-How-Many-Seniors-Live-in-Poverty.
33 Karan Manke, Racial Discrimination Linked to Higher Risk of Chronic Illness in African American Women, Berkeley News (Oct. 5, 2018), https://news.berkeley.edu/2018/10/05/racial-discrimination-linked-to-higher-risk-of-chronic-illness-in-african-american-women/.
34 L. Balcázar-Hernández et al., Women and COVID-19: Severity and Mortality in Hospitalized Middle-Aged and Older Patients, 24 Climacteric 313 (2021), https://pubmed.ncbi.nlm.nih.gov/33513033/.
35 Carole H. Sudre et al., Attributes and Predictors of Long COVID, 27 Nature Medicine 626 (2021), https://www.nature.com/articles/s41591-021-01292-y (finding that long COVID was more likely with increasing age and among women); Ingrid Torjesen, BMJ, Covid-19: Middle Aged Women Face Greater Risk of Debilitating Long Term Symptoms (March 25, 2021), https://www.bmj.com/content/372/bmj.n829 (finding that long COVID symptoms were more prevalent in women 50-60 years old).
36 Jill Diesel et al., COVID-19 Vaccination Coverage Among Adults — United States, December 14, 2020–May 22, 2021, 70 Morbidity and Mortality Weekly Report 922 (June 2021), https://www.cdc.gov/mmwr/volumes/70/wr/mm7025e1.htm.
37 Brittni Frederiksen, Usha Ranji, Alina Salganicoff, & Michelle Long, Kaiser Family Found, Women’s Experiences with Health Care During the COVID-19 Pandemic: Findings from the KFF Women’s Health Survey (March 2021), https://www.kff.org/womens-health-policy/issue-brief/womens-experiences-with-health-care-during-the-covid-19-pandemic-findings-from-the-kff-womens-health-survey/.
38 Id.
39 Mary Beth Musumeci, Priya Chidambaram, & Molly O’Malley Watts, Kaiser Family Found., Medicaid Financial Eligibility for Seniors and People with Disabilities: Findings from a 50-State Survey (Jun. 2019), https://www.kff.org/report-section/medicaid-financial-eligibility-for-seniors-and-people-with-disabilities-findings-from-a-50-state-survey-issue-brief/.
40 Arizona Health Care Costs Containment System (AHCCCS), Eligibility Requirements (February 1, 2021), https://www.azahcccs.gov/Members/Downloads/EligibilityRequirements.pdf.
41 Medicare Rights Center, Medicare Savings Program Financial Eligibility Guidelines (2018), medicareinteractive.org/pdf/MSPFinancialEligibiltyGuidelines.pdf.
42 AARP Public Pol’y Inst., AARP Nursing Home COVID-19 Dashboard (Sept. 15, 2021), https://www.aarp.org/ppi/issues/caregiving/info-2020/nursing-home-covid-dashboard.html.
43 Rebecca J. Gorges & R. Tamara Konetzka, Factors Associated with Racial Differences in Deaths Among Nursing Home Residents with COVID-19 Infection in the US, 4 JAMA Network Open 1 (2021), https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2776102.
44 Amber Christ & Natalie Kean, Justice in Aging, Medicaid Home and Community-Based Services for Older Adults with Disabilities: A Primer (Apr. 2021), https://justiceinaging.org/wp-content/uploads/2021/04/HCBS-Primer.pdf.
45 Agency for Healthcare Rsch. and Quality, Assessing the Health and Welfare of the HCBS Population (Dec. 2021), https://www.ahrq.gov/patient-safety/settings/long-term-care/resource/hcbs/findings/find5.html.
46 Victoria Peebles et al., Mathematica Pol’y Rsch., HCBS Claims Analysis Chartbook: Final Report 68 (Dec. 2017), https://www.mathematica.org/publications/hcbs-claims-analysis-chartbook-final-report.
47 Chanee D. Fabius et al., Racial Disparities in Medicaid Home and Community-based Service Utilization and Expenditures Among Persons with Multiple Sclerosis 18 BMC Health Serv’s Rsch. 1 (Oct. 2018), https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-018-3584-x
48 Chanee D. Fabius, Jessica Ogarek, & Theresa I. Shireman, Racial Disparities in Medicaid Home and Community-Based Service Utilization among White, Black, and Hispanic Adults with Multiple Sclerosis: Implications of State Policy 6 J. Racial Ethnic Health Disparities 1200 (June 2019), https://pubmed.ncbi.nlm.nih.gov/31359384/.
49 Rachel Fehr et al., Kaiser Family Found., Mapping Pre-existing Conditions Across the U.S. (Aug. 2018), https://www.kff.org/health-reform/issue-brief/mapping-pre-existing-conditions-across-the-u-s/.